
Case Study Series
NanoHive Medical HiveTM Standalone ALIF System
Jaideep Chunduri, MD
Orthopaedic Spine Surgeon
Cincinnati, OH

Technology Background
The use of interbody fusion cages, including anterior lumbar interbody fusion (ALIF) cages, in the treatment of spondylolisthesis and spinal deformity is common and understanding factors affecting successful fusion is critical to improving outcomes.
One of the most commonly employed techniques for achieving fusion is implantation of an interbody cage. A study from the Nationwide Inpatient Sample database showed as many as 83% of surgeries for degenerative spondylolisthesis involve the use of an interbody cage [1]. Titanium was first used in interbody cages because it enhanced cell adhesion and osseointegration favoring bone fusion [2], however, it may have had a higher rate of subsidence compared to polyetheretherketone (PEEK) due to differences in the modulus of elasticity [3,4]. Despite that, PEEK is chemically inert with limited cell adhesion and fixation to bone [5].
Advocates for PEEK devices have recognized the need for reduced stiffness, as compared to subtractively manufactured titanium implants; however, PEEK lacks the beneficial cellular characteristics of titanium. Titanium surfaces where manufacturers can control tissue interaction to the nano-scale may offer even greater advantages.
Frequently, titanium 3D printed implants rely on rigid framed structures, shells, and solid noses and tails to bear the loads required for rigorous mechanical performance demands. The result increases construct stiffness and reduces load on internal bone graft.
Alternate approaches to internal porosity utilize randomly generated structures prone to unknown failure points, inconsistent or reduced bone loading, and to choke points for fluid flow. Truss structures may be prone to loss of graft material, particularly during insertion, and may not provide substantial surface area to support tissue during healing.
The design goals for the Hive™ implant, with Soft Titanium® technology, were to offer a powerful feature set, including:
- a supporting scaffold for bone growth
- ideal pore characteristics for ingrowth
- maximal surface for bone to attach
- post-operative visibility
- and mechanical compatibility
As a result, the Hive scaffold has an overall stiffness comparable to PEEK. Mechanical performance testing for spine implants is conducted in accordance with ASTM F2077 for evaluation of the axial strength and stiffness of the tested device modulus.
Soft Titanium, with modulus of elasticity and stiffness that is matched closely to normal bone, has two potential advantages for obtaining solid fusion after spine surgery. One advantage is the potential benefit of allowing some elastic deformation during regular activities, which in turn will place more loading on the healing fusion without destabilizing the construct and may influence improved bone formation at the fusion site. The second potential advantage of a lower stiffness cage is a lower risk of subsidence, especially in osteoporotic patients, which may prevent compromised fixation and loss of correction. This loss of correction can impact alignment and indirect decompression, subsequently negatively affecting clinical outcomes. A cage with lower stiffness is also potentially less likely to violate the endplates on insertion, which can also prevent subsidence.
The purpose of this study is to report on one surgeon’s experience with the Soft Titanium technology in a standalone ALIF cage.
Methods
Twenty-six Anterior Lumbar Interbody Fusion (ALIF) cases, from March 1, 2021 to December 14, 2021, were retrospectively reviewed. Fifty-eight percent were male. The average age was 56 years old (range 31 – 71) and the average BMI was 29.9 (range 19.0 – 38.9). A total of forty-four cages were placed. Twenty-five were placed at L5-S1, sixteen were placed at L4-L5 and three were placed at L3-L4.
All patients were classified as non-smoking at the time of the initial operation and indications for surgery were combinations of degenerative disc disease, stenosis, spondylolisthesis and reoccurrent disc herniation. One patient had degenerative scoliosis and flat back.
Anterior exposures were performed by an experienced vascular surgeon, with over 10,000 cases performed. All cages were placed in the direct anterior approach. Bone graft was placed in the central lumen of the cage, as well as injected in the ports located within lateral walls of the implant. With the exception of two cases, all posterior decompressions and fusions were performed using an open procedure. Surgery time was typically under 3.5 hrs, which included the time needed to switch to the posterior approach for the addition of pedicle screws. Although the NanoHive Standalone ALIF cage is approved as a standalone device, posterior pedicle screws were added to increase stability to the construct. This is especially useful when a complete facetectomy is necessary for decompression.
Typical hospital stay was 2-3 days, with no infections and no prolonged ileus (greater than 2 days).
Results
All twenty six patients who had the anterior lumbar interbody fusion (ALIF) procedure were seen at 1, 3, 6, and 12 months post-op.
- Fusion was assessed by examining radiographs for lucencies around the pedicle screws, cage screws, or the cage itself, as well as motion on flexion / extension radiographs.
- At 12 months, there were no reoperations at the index levels and all patients were assessed as fused at each level.
Conclusions
- The Hive Standalone ALIF System, from NanoHive Medical, is a simple to use, 3-D printed titanium implant with a large bone graft window and the ability to inject through the central lumen and sidewalls of the cage.
- Multiple implant options, from a width and depth perspective, as well as variable degrees of lordosis, allow for matching of patient anatomy.
- The implant can be placed with or without the use of an all-in-one drill guide.
- This has been a successful implant in this surgeon’s practice.
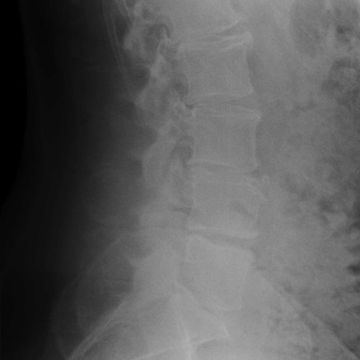
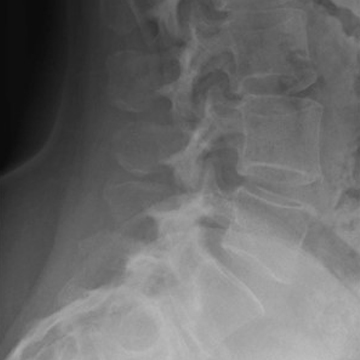
Patient #1
A 58 year old female with chronic low back pain that worsened after a motor vehicle accident.
—
The patient had a previous lumbar fusion at L5-S1, as well as a discectomy at L4-5. Radiographs revealed a spondylolisthesis at L4-5. She was osteopenic and had a BMI of 28.
—
An MRI revealed stenosis at L4-5 and L5-S1 and a CT scan showed a pseudoarthrosis/no evidence of fusion at L5-S1.
—
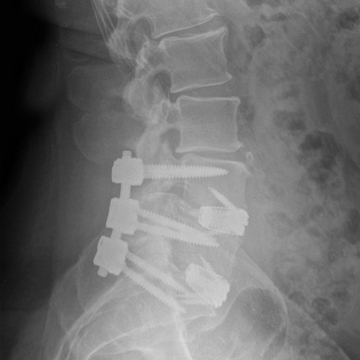
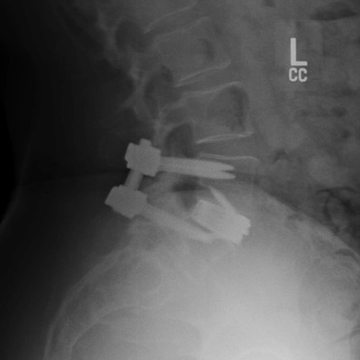
The patient elected to undergo an anterior lumbar interbody fusion (ALIF) with posterior fixation at L4-5 and L5-S1 levels.
—
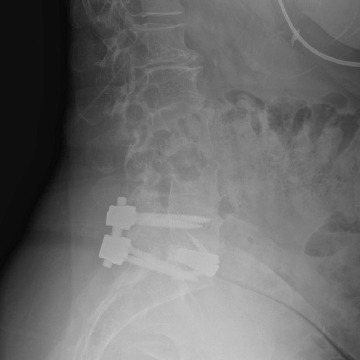
At 6 months, the patient reported significant reduction in pain and resumed all normal activities.

Pre-Op

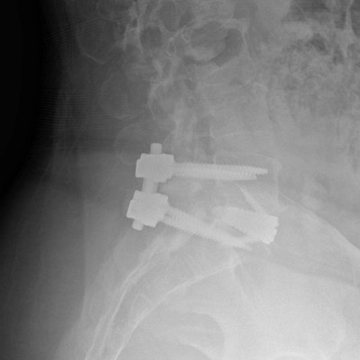
6 Weeks

6 Months
Patient #2
A 65 year old male with a history of chronic progressive low back pain with significant radiculopathy. He had normal bone density and a BMI of 37.
—
SI joint injections were attempted but x-rays eventually showed significant progression of the spondylolisthesis at L4-5.
—
An MRI showed evidence of Modic Type 2 changes at L5-S1, along with severe facet arthropathy at L4-5 with instability. There was no significant stenosis.
—
An anterior lumbar interbody fusion with posterior fixation was recommended from L4-S1 due to the severity of the disc degeneration and the ability to do a posterior minimally invasive fusion in the back.
—
At 3 months, the patient stated that his back was as good as it had ever been in the previous ten years.

Pre-Op

6 Weeks

6 Months

12 Months
Patient #3
A 45 year old male with a previous left sided decompression at L4-5 and L5-S1, with multi-level stenosis on the left side from L3-S1. He had a BMI of 34 and normal bone density.
—
The patient had failed all conservative care and had progressive back and left leg pain.
—
An MRI revealed recurrent stenosis at L4-5 and L5-S1, with moderate foraminal stenosis at L3-4.
—
Due to the significant recurrence as well as the multilevel degenerative disc disease, the patient elected to undergo a two level anterior lumbar interbody fusion (ALIF) with posterior fixation from L4-S1 with a decompression at L3-4.
—
At 4 months, he was pain free and returned to work.
Pre-Op

6 Weeks

6 Months
12 Months
Patient #4
A 56 year old female with a long standing history of back and left leg pain for 18 months. She had a history of scoliosis, was osteopenic, and had a BMI of 31.
—
An MRI of the lumbar spine showed severe foraminal stenosis at L5-S1, with degenerative disc disease.
—
She elected to have anterior lumbar fusion with posterior fixation at L5-S1 level.
—
She was pain free at 3 months postoperative and resumed all normal activity at 6 months.

Pre-Op
6 Weeks

6 Months
12 Months
Patient #5
A 54 year old female with a one year history of back and right leg pain that failed conservative care. She had a BMI of 32 and normal bone density.
—
An MRI revealed a Grade 1 spondylolisthesis with severe facet arthropathy, with a large right sided facet cyst at L4-5.
—
The patient elected to have an anterior lumbar interbody fusion at L4-5 due to the instability and the need to decompress the facet cyst.
—
She was pain free at 3 months and resumed all normal activity at 6 months.
Pre-Op

6 Weeks
6 Months
1. Norton RP, Bianco K, Klifto C, et al. Degenerative spondylolisthesis: an analysis of the nationwide inpatient sample database. Spine (Phila Pa 1976) 2015;40:1219–27
2. Kuslich SD, Ulstrom CL, Griffith SL, et al. The Bagby and Kuslich method of lumbar interbody fusion. History, techniques, and 2-year follow-up results of a United States prospective, multicenter trial. Spine (Phila Pa 1976) 1998;23:1267–78
3. Chou YC, Chen DC, Hsieh WA, et al. Efficacy of anterior cervical fusion: comparison of titanium cages, polyetheretherketone (PEEK) cages and autogenous bone grafts. J Clin Neurosci. 2008;15:1240–5. [PubMed] [Google Scholar]
4. Chen Y, Wang X, Lu X, et al. Comparison of titanium and polyetheretherketone (PEEK) cages in the surgical treatment of multilevel cervical spondylotic myelopathy: a prospective, randomized, control study with over 7-year follow-up. Eur Spine J. 2013;22:1539–46.
5. Kurtz SM, Devine JN. PEEK biomaterials in trauma, orthopedic, and spinal implants. Biomaterials. 2007;28:4845–69